Myoglobin, cardiac Troponin I (cTnI), and NT-proBNP get grouped together as "cardiac biomarkers," but they answer three different clinical questions on three different timelines. Two of them — myoglobin and cTnI — compete for the same job of detecting acute myocardial injury as early and reliably as possible. The third, NT-proBNP, is not measuring ischemic injury at all; it is measuring ventricular wall stress, and ordering it to rule in or rule out a heart attack is a category error that shows up more often than IVD developers might expect.
This guide lines up the onset, peak, and clinical role of all three biomarkers, walks through why myoglobin's clinical footprint has narrowed as high-sensitivity troponin assays have matured, and explains exactly where NT-proBNP fits into an acute cardiac workup instead.
1. Why Compare Myoglobin, cTnI & NT-proBNP?
All three markers are released by cardiac tissue under stress, but the type of stress and the resulting kinetic signature are fundamentally different. Myoglobin and cTnI are both intracellular structural or enzymatic proteins that leak into circulation only when cardiomyocytes are physically damaged — they are markers of necrosis. NT-proBNP, by contrast, is actively synthesized and secreted by ventricular myocytes in response to mechanical stretch from pressure or volume overload — it is a marker of strain, not death, and it rises in chronic heart failure even when no acute injury has occurred at all.
That distinction is why a well-designed acute cardiac panel does not simply average or rank these three markers by speed. It uses myoglobin and cTnI together to answer "has a myocardial infarction occurred," and adds NT-proBNP separately to answer "is this dyspnea cardiac, and how much ventricular strain is present" — two different questions that happen to share the word "cardiac."
Critical Principle
Injury markers (myoglobin, cTnI) and strain markers (NT-proBNP) are not interchangeable and are not competing for the same diagnostic slot. Ordering NT-proBNP to rule out AMI, or ordering troponin alone to assess heart failure severity, both miss the biomarker's intended clinical question.
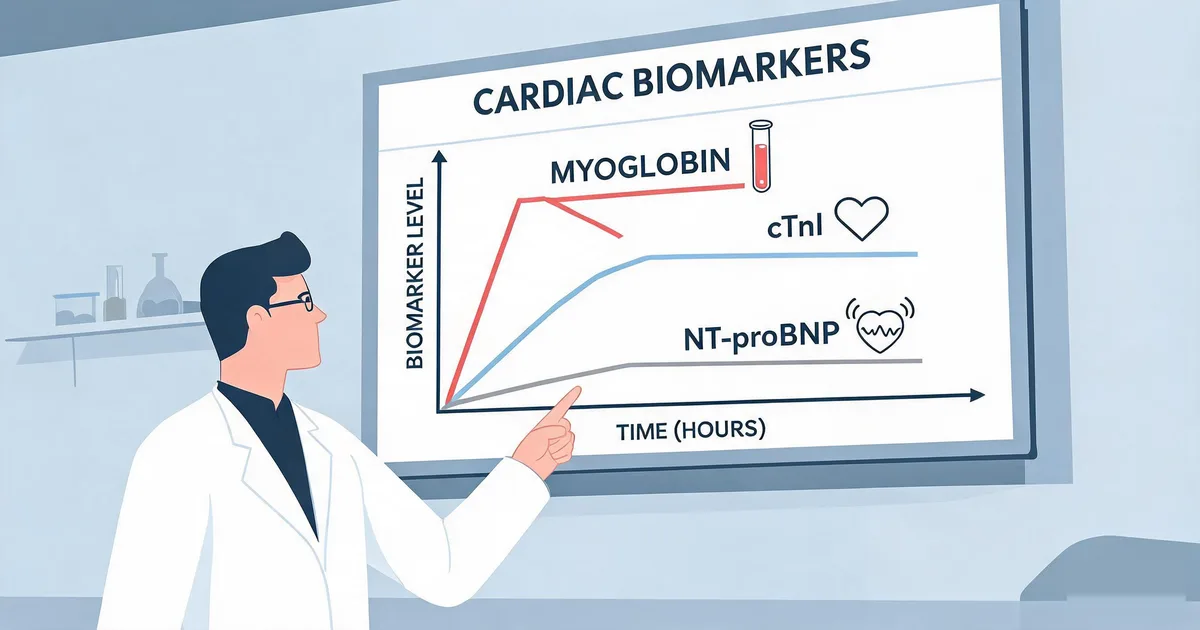
2. Kinetics Compared: Onset, Peak & Clearance
Among the two injury markers, the difference in release kinetics comes down to molecular size and cellular location: myoglobin is a small (17.8 kDa) cytoplasmic protein that diffuses into blood quickly, while troponin is bound in the contractile apparatus and releases more gradually, first from a small cytosolic pool and then progressively as the structural complex breaks down.
| Marker | Onset | Peak | Duration Elevated | Biological Role |
|---|---|---|---|---|
| Myoglobin | 1–3 hours | 6–9 hours | ~24 hours | Cardiac + skeletal muscle injury |
| cTnI | 2–6 hours | 12–24 hours | 5–10 days | Cardiac-specific injury |
| NT-proBNP | Hours (proportional to strain) | Varies with severity | Persists while strain continues | Ventricular wall stress |
The duration-elevated column is where the clinical trade-off becomes obvious. Myoglobin's fast clearance makes it useful for detecting reinfarction — a second injury can be seen as a new rise superimposed on a marker that has already returned toward baseline — but it also means a patient who presents more than 24 hours after symptom onset can have a falsely reassuring myoglobin result despite a confirmed AMI. cTnI's much longer elevation window (5–10 days) makes it the marker of choice for retrospective diagnosis in patients who delay seeking care, at the cost of being less useful for distinguishing a new event from a recent one without a clean baseline.
3. Myoglobin: The Early, Non-Specific Signal
Myoglobin's defining clinical property is speed: it is released into circulation within 1–3 hours of ischemic onset, faster than any other routinely used cardiac biomarker, and reaches peak concentration (typically 50–100× the normal 28–72 ng/mL reference range) at 6–9 hours. In the earliest hours of chest pain presentation — before troponin has had time to rise appreciably — a negative myoglobin result carries meaningful rule-out value.
The trade-off is specificity. Myoglobin is expressed in both cardiac and skeletal muscle, so any source of muscle injury — strenuous exercise, intramuscular injection, trauma, rhabdomyolysis, or polymyositis — elevates it independent of cardiac status. Reduced renal clearance in patients with kidney impairment further inflates baseline levels. For this reason, myoglobin is never used as a stand-alone diagnostic marker; its role is strictly as the early-window component of a multi-marker panel, always interpreted alongside cTnI rather than in place of it.
- Best use case: earliest possible signal in a 0–4 hour chest pain presentation, particularly where high-sensitivity troponin is not available.
- Limitation: non-specific to cardiac tissue; a positive result requires troponin confirmation, and a negative result late in the clinical course does not reliably exclude AMI.
- IVD relevance: the Sekbio myoglobin antibody pair (GSA501 capture + GSA503 detection) is validated for LFA-FIA and CLIA formats against the Roche Elecsys ECLIA reference assay across a 25–3,000 ng/mL clinical range.
4. cTnI: The Diagnostic Gold Standard
Cardiac Troponin I is the reference biomarker for AMI diagnosis under ESC and ACC/AHA guidelines because it combines high cardiac specificity with a wide diagnostic window. Conventional-sensitivity assays detect a rise within 2–6 hours of injury, with peak concentration at 12–24 hours and measurable elevation persisting for 5–10 days — long enough to confirm a myocardial infarction retrospectively in a patient who delayed presentation, something myoglobin's fast clearance cannot do.
Troponin's cardiac specificity comes from isoform differences between skeletal and cardiac muscle: unlike myoglobin, cTnI released from cardiomyocytes is structurally distinct from skeletal troponin I, so a well-designed antibody pair does not cross-react with skeletal muscle injury. This is what makes an isolated troponin elevation a much stronger signal of cardiac-specific damage than an isolated myoglobin elevation.
"Myoglobin answers 'has anything happened yet' in the first few hours; cTnI answers 'was it the heart' with a diagnostic window measured in days, not hours — which is why troponin, not myoglobin, remains the reference standard AMI markers are judged against."
Assay sensitivity matters most at the low end of the troponin range, since the clinical decision threshold sits close to the limit of detection. High-sensitivity troponin (hs-cTnI) platforms resolve concentrations an order of magnitude lower than conventional assays, which is what enabled the shortened 0/1h and 0/3h rule-out protocols in Section 6. The Sekbio cTnI antibody pair supports a CLIA format (0.001–35.97 ng/mL, blank LoD 0.0032 ng/mL) and an FIA format (0.1–40 ng/mL, LoD 0.1 ng/mL), validated against Abbott ARCHITECT across 60 clinical samples.
5. NT-proBNP: A Different Question Entirely
NT-proBNP is the 76-amino acid, biologically inactive N-terminal fragment cleaved from proBNP-108 when ventricular myocytes are stretched under pressure or volume overload. It is released in equimolar amounts alongside the active hormone BNP, but its plasma half-life (60–120 minutes) is substantially longer than BNP's (~20 minutes), which is why NT-proBNP, not BNP, is the more common immunoassay target — the longer half-life produces a more stable, easier-to-interpret result.
Critically, NT-proBNP does not indicate myocardial necrosis. A patient can have a markedly elevated NT-proBNP from chronic heart failure with no acute ischemic event at all, and a patient in the earliest hours of an AMI without existing ventricular strain can have a normal NT-proBNP. This is why NT-proBNP is ordered for a categorically different clinical scenario than myoglobin or troponin: differentiating cardiac dyspnea (heart failure) from pulmonary dyspnea, and staging the severity of ventricular strain once heart failure is confirmed.
| Clinical Scenario | Age Group | Acute HF Cutoff |
|---|---|---|
| Acute heart failure diagnosis | <50 years | 450 pg/mL |
| Acute heart failure diagnosis | 50–75 years | 900 pg/mL |
| Acute heart failure diagnosis | >75 years | 1,800 pg/mL |
| Chronic heart failure diagnosis | All ages | 125 pg/mL |
These age-stratified cutoffs exist because NT-proBNP rises with age-related declines in ventricular compliance and renal clearance independent of any acute cardiac event — a drift troponin, as a marker of a discrete injury, does not share. NT-proBNP calibration therefore requires age-aware interpretation rather than a single-threshold approach. Sekbio's NT-proBNP antibody panel covers 7 mouse monoclonal antibodies across epitopes 13–76 plus a humanized variant, supporting non-overlapping capture/detection pairs calibrated to these thresholds.
6. Rule-Out Algorithms in Practice
How these three markers get combined depends heavily on which troponin assay generation is available on a given platform:
- High-sensitivity troponin available: ESC-endorsed 0/1h or 0/3h algorithms draw a baseline hs-cTnI sample and a second sample 1–3 hours later, using the absolute value and the delta between draws to classify patients as rule-out, observe, or rule-in. Because hs-cTnI detects meaningful changes within this shortened window, myoglobin's role as the fastest-available signal has largely been absorbed by troponin itself.
- Conventional-sensitivity troponin only: myoglobin retains value as the earlier-window component of a 2-hour AMI rule-out panel (myoglobin + cTnI, sometimes CK-MB), particularly where a high-sensitivity CLIA platform is not accessible.
- Dyspnea of unclear cause: NT-proBNP is added independent of the troponin protocol, specifically to separate cardiac (heart failure) from non-cardiac (pulmonary) causes — it does not substitute for myoglobin or troponin in the ischemia work-up.
- Renal impairment: both cTnI and NT-proBNP require cautious interpretation, since reduced clearance elevates baseline concentrations of each independent of cardiac status; serial trending matters more than a single value here.
IVD Application Note
Multiplex acute cardiac panels combining myoglobin, cTnI, and NT-proBNP on a single LFA strip or CLIA run allow a single blood draw to answer both the injury question and the strain question simultaneously, reducing turnaround time in emergency department triage versus ordering the tests sequentially. See the cardiac biomarker antibody products overview for the full panel matrix.
7. Assay & Panel Design Considerations
Building a combined myoglobin/cTnI/NT-proBNP panel introduces requirements beyond running three independent single-marker assays side by side:
- Dynamic range mismatch: myoglobin circulates at ng/mL concentrations in the tens to thousands, cTnI spans near-zero to tens of ng/mL, and NT-proBNP is reported in pg/mL up to the tens of thousands in severe heart failure — three working ranges that typically require separate detection channels or reagent concentrations.
- Low-end precision for troponin: because the cTnI decision zone sits close to the limit of detection, single-digit within-run CV at low concentrations is necessary to distinguish a real trend from analytical noise in serial hs-cTnI monitoring.
- Cross-reactivity screening: myoglobin and cTnI antibody pairs must each be validated against skeletal muscle isoforms of their targets, since that specificity gap is what separates a cardiac-relevant result from a false positive.
- Format choice by care setting: CLIA analyzers suit centralized labs running serial hs-cTnI trends; LFA-FIA point-of-care formats suit emergency departments and ambulance triage needing a same-visit rule-out decision.
8. Summary
Comparing myoglobin, cTnI, and NT-proBNP comes down to recognizing that only two of the three are answering the same question:
- Myoglobin: fastest onset (1–3h), fastest clearance (~24h), not cardiac-specific — best as an early-window component alongside cTnI, with a shrinking role as hs-cTnI adoption expands.
- cTnI: slower onset (2–6h) but cardiac-specific and elevated for 5–10 days — the diagnostic reference standard for AMI, and the anchor of 0/1h and 0/3h rule-out algorithms.
- NT-proBNP: a strain marker, not an injury marker — used to differentiate cardiac from non-cardiac dyspnea and stage heart failure severity, with age-stratified rather than single-threshold cutoffs.
- Combined panels add clinical value specifically when both the injury question and the strain question are open at once, such as ACS presentations with suspected concurrent heart failure or renal impairment.
At Sekbio, we manufacture the monoclonal antibody pairs behind all three of these assays, each independently validated against reference platforms for CLIA and LFA-FIA sandwich immunoassay development. If you are building a single-marker assay or a combined acute cardiac panel, our team can walk through reagent-level performance data for your specific platform.
Frequently Asked Questions — Cardiac Biomarker Kinetics
What is the main difference between myoglobin, cTnI, and NT-proBNP as cardiac biomarkers?
Myoglobin and cTnI both detect acute myocardial injury but on different timelines: myoglobin rises fastest (1–3 hours) but is not cardiac-specific, while cTnI rises slower (2–6 hours) but is the specificity gold standard and stays elevated for 5–10 days. NT-proBNP answers a different clinical question entirely — it reflects ventricular wall stress from heart failure rather than myocardial necrosis, so it is used to differentiate cardiac from pulmonary causes of dyspnea, not to diagnose a heart attack.
Why isn't myoglobin used alone to diagnose a heart attack?
Myoglobin is present in both cardiac and skeletal muscle, so any skeletal muscle injury, intramuscular injection, strenuous exercise, or reduced renal clearance can elevate it without any cardiac event occurring. It also returns to baseline within about 24 hours, so a delayed presentation can produce a false-negative myoglobin result even in a confirmed AMI. Myoglobin's clinical value is as an early, sensitive rule-out signal alongside cTnI, not as a stand-alone diagnostic marker.
How do 0/1h and 0/3h high-sensitivity troponin algorithms use these kinetics?
ESC-endorsed rapid rule-out/rule-in protocols draw a baseline high-sensitivity cTnI sample at presentation and a second sample 1 or 3 hours later, using both the absolute value and the delta (change) between the two draws to classify patients as rule-out, observe, or rule-in. High-sensitivity troponin assays can detect clinically meaningful rises within this shortened window, which is why myoglobin's historical role as the earliest-available signal has narrowed to settings where a high-sensitivity troponin platform is not available.
When should NT-proBNP be ordered instead of, or alongside, troponin?
NT-proBNP is ordered when the clinical question is heart failure rather than acute ischemia — most commonly in patients presenting with dyspnea, where it helps distinguish a cardiac cause from a pulmonary one. It is also drawn alongside troponin in acute coronary syndrome when concurrent heart failure or ventricular strain is suspected, and in patients with renal impairment where cTnI interpretation can be complicated by reduced clearance.
Why does NT-proBNP have age-stratified cutoffs while troponin does not?
NT-proBNP rises with age-related changes in ventricular compliance and renal clearance independent of acute cardiac injury, so a single cutoff would over-diagnose heart failure in older patients. ESC guidelines therefore stratify acute heart failure cutoffs by age (450 pg/mL under 50 years, 900 pg/mL for 50–75 years, 1,800 pg/mL over 75 years), while a single 99th-percentile cutoff is used for troponin because it reflects a discrete injury event rather than a continuous physiological variable.
Does Sekbio supply antibody pairs for myoglobin, cTnI, and NT-proBNP panel development?
Yes. Sekbio manufactures validated monoclonal antibody pairs for myoglobin, cTnI, and NT-proBNP, each independently validated for CLIA and LFA-FIA sandwich immunoassay formats and benchmarked against reference platforms such as Roche ECLIA and Abbott ARCHITECT. Explore the individual datasheets or discuss a combined acute cardiac panel through our antibody development services.