CRP, procalcitonin (PCT), and IL-6 are often described interchangeably as "inflammatory markers," but they answer different clinical questions on different timelines. Ordering the wrong one — or reading a single result without accounting for its kinetics — is a common source of diagnostic delay in suspected sepsis.
This guide lines the three biomarkers up directly: how fast each one rises, how long each stays elevated, how specific each is to bacterial infection, and the two scenarios where testing more than one at once genuinely changes the diagnostic picture.
1. Why Compare CRP, PCT & IL-6?
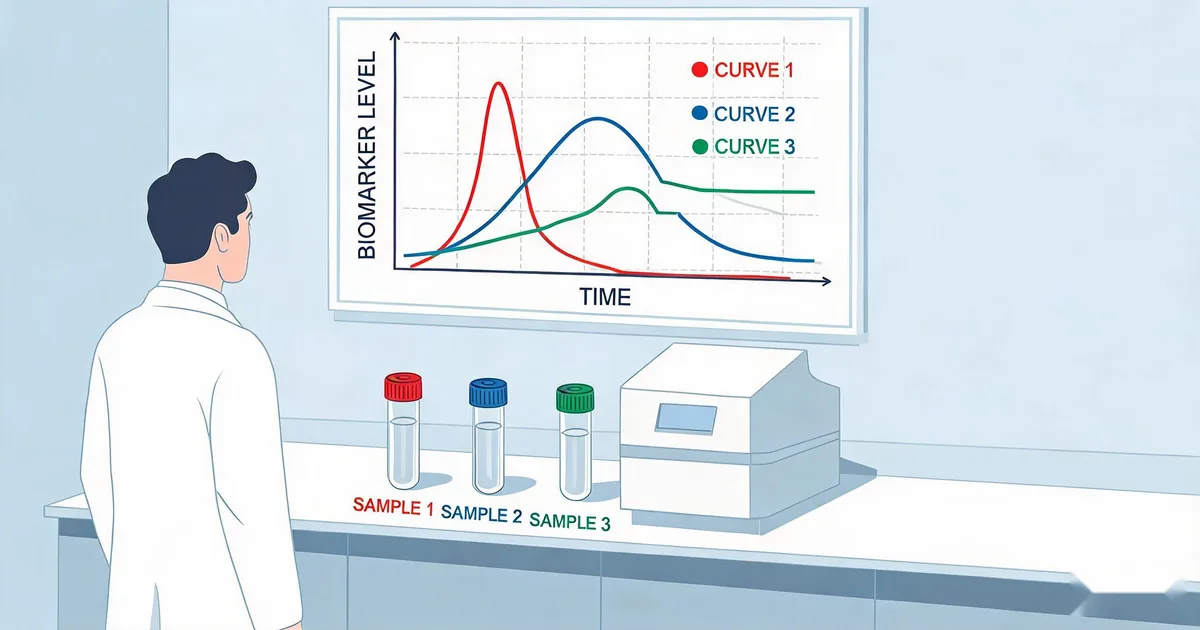
All three markers rise as part of the same inflammatory cascade, but at different points in the sequence. IL-6 is an early cytokine released directly by immune cells at the site of infection. It then travels to the liver and drives hepatic synthesis of CRP — meaning CRP's rise is downstream of, and delayed relative to, IL-6's rise. PCT sits kinetically between the two: it is released by extrathyroidal tissues in response to bacterial endotoxin, independent of the IL-6-to-CRP pathway, which is part of why it tracks bacterial infection more specifically than CRP does.
Understanding this sequence — cytokine signal (IL-6) → bacterial-specific response (PCT) → downstream acute-phase protein (CRP) — explains why the three markers behave so differently in the same patient at the same moment, and why choosing the right one depends on how many hours have elapsed since the infection started.
Critical Principle
None of these three markers is "better" in an absolute sense — each is optimized for a different point on the infection timeline. Interpreting any single value without knowing where the patient sits on that timeline is the most common source of misread results.
2. Kinetics Compared: Onset, Peak & Half-Life
The three markers differ substantially in how quickly they respond and how quickly they clear:
| Marker | Onset | Peak | Plasma Half-Life | Source |
|---|---|---|---|---|
| IL-6 | 1–2 hours | 4–6 hours | ~1 hour | Immune cells (cytokine) |
| Procalcitonin (PCT) | 2–4 hours | 6–24 hours | ~24 hours | Extrathyroidal tissues (endotoxin-driven) |
| CRP | 6–8 hours | 24–48 hours | ~19 hours | Liver (IL-6-driven synthesis) |
Half-life explains why each marker behaves the way it does in serial monitoring. IL-6's ~1-hour half-life means its concentration reflects the real-time rate of cytokine release — it can spike and fall within the same day, which makes it sensitive to rapid changes but harder to interpret from a single delayed sample. CRP's much longer, comparatively stable ~19-hour half-life means its level mainly reflects cumulative synthesis, so it declines slowly even after the underlying stimulus has stopped — useful for tracking overall inflammatory burden over days, less useful for detecting a change that happened six hours ago. PCT's ~24-hour half-life sits close to CRP's, which is why the PCT-guided antibiotic stewardship algorithm uses 24–48 hour serial monitoring intervals rather than same-day retesting.
3. Diagnostic Specificity: Bacterial vs. Non-Bacterial Inflammation
Speed is only half the picture — how selectively each marker responds to bacterial infection versus other causes of inflammation also differs substantially:
- PCT is the most bacterial-specific of the three. It stays comparatively low in viral infection, autoimmune flares, and most non-infectious tissue injury, which is why it anchors antibiotic initiation and discontinuation decisions.
- CRP is the least specific. It rises with bacterial infection, viral infection, autoimmune disease activity, surgical trauma, and malignancy alike — a high CRP raises suspicion for inflammation broadly but does not by itself point to a bacterial cause.
- IL-6 sits in between: it is a broad upstream signal of acute inflammation (infectious or not), but because it also drives the intensity of the downstream CRP and PCT response, an unusually high IL-6 relative to CRP/PCT can flag a very early or very severe inflammatory event before the other two have caught up.
"Speed and specificity trade off in opposite directions across these three markers — IL-6 is fastest but least specific to bacterial cause, PCT is the most bacterial-specific, and CRP is the slowest but cheapest and most universally available."
4. When a Single Marker Is Enough
Most clinical workflows do not need all three markers simultaneously. A single marker is usually sufficient when:
- General inflammation screening >8 hours from onset: CRP alone is adequate and is the cheapest, most widely available option on standard lab platforms.
- Antibiotic initiation/discontinuation decisions: PCT alone, following the four-tier cutoff algorithm, is the validated approach — see the dedicated PCT-guided antibiotic stewardship guide for the full protocol.
- Serial ICU trending over multiple days: PCT's stable clearance profile makes single-marker serial trending straightforward without needing IL-6's rapid fluctuation to interpret.
5. When Combination Testing Adds Value
Combination testing earns its added cost and complexity in two specific scenarios:
- Early presentation (<6 hours from symptom onset): CRP and, to a lesser extent, PCT may not yet be meaningfully elevated even in confirmed bacterial infection. IL-6 is more likely to already be elevated at this stage, so adding it improves early sensitivity in emergency-department triage before CRP or PCT would otherwise flag the case.
- The CRP diagnostic gray zone (roughly 20–100 mg/L): at these intermediate levels, CRP alone cannot reliably separate bacterial infection from viral illness, autoimmune flares, or post-surgical inflammation. Adding PCT narrows the differential by testing bacterial specificity directly, rather than inflammatory burden generally.
Outside these two windows, adding a second or third marker tends to improve statistical performance only marginally while adding cost and turnaround time — the incremental diagnostic gain from a three-marker panel is largest precisely where a single marker's blind spot (early timing for CRP/PCT, or non-specificity for CRP) would otherwise cause a missed or delayed call.
IVD Application Note
Sekbio supplies pre-validated monoclonal antibody pairs for CRP, PCT, and IL-6, each independently validated in sandwich immunoassay format, for developers building single-marker or combined sepsis panel assays.
6. Assay & Panel Design Considerations
Building a combined panel introduces requirements beyond simply running three independent single-marker assays side by side:
- Dynamic range mismatch: CRP circulates at mg/L concentrations, while PCT and IL-6 circulate at ng/mL and pg/mL levels respectively — three to six orders of magnitude apart — so a shared platform needs either separate detection channels or very different reagent concentrations per target.
- Turnaround time alignment: if the clinical goal is a single-visit triage decision, all three assays need comparable turnaround (typically CLIA or FIA formats under 30 minutes) so the panel result arrives as one actionable data point rather than staggered over hours.
- Cross-reactivity screening: antibody pairs for structurally distinct targets like CRP, PCT, and IL-6 have low intrinsic cross-reactivity risk with each other, but each pair must still be individually validated against the sample matrix (serum, plasma, or whole blood) intended for the panel.
- Reference interval by assay platform: IL-6 in particular shows meaningful assay-to-assay variability in reported units and cutoffs, so panel developers should validate cutoffs on their own platform rather than importing values directly from literature run on a different analyzer.
7. Summary
Choosing between CRP, PCT, and IL-6 — or combining them — comes down to timing and specificity:
- IL-6: fastest onset (1–2h), fastest clearance (~1h half-life), least bacterial-specific — best for very early detection.
- PCT: intermediate onset (2–4h), stable ~24h half-life, most bacterial-specific — best for antibiotic initiation and discontinuation decisions.
- CRP: slowest onset (6–8h), long ~19h half-life, least specific but cheapest and most available — best for general inflammation screening and multi-day trending.
- Combine markers specifically for early (<6h) presentations or when CRP falls in the 20–100 mg/L gray zone — outside those windows, a single well-chosen marker is usually sufficient.
At Sekbio, we manufacture the antibody pairs behind all three of these assays, individually validated for CLIA, FIA, and ELISA formats. If you're designing a single-marker assay or a combined sepsis panel, our team can walk through reagent-level performance data for your specific platform.
Frequently Asked Questions — CRP, PCT & IL-6 Kinetics
What is the main difference between CRP, procalcitonin, and IL-6 as inflammatory biomarkers?
IL-6 rises earliest (within 1-2 hours) but clears fastest and is less specific to bacterial infection. Procalcitonin (PCT) rises within 2-4 hours, is more specific to bacterial infection, and has a stable 24-hour half-life suited to serial trending. CRP rises slowest (6-8 hours), stays elevated longest, and is the least specific of the three, also rising in viral infection, autoimmune disease, and tissue injury.
Which biomarker rises fastest after a bacterial infection starts?
IL-6 rises fastest, detectable within 1-2 hours of the inflammatory stimulus and peaking around 4-6 hours, because it is an upstream cytokine that directly triggers hepatic CRP synthesis. PCT follows at 2-4 hours, and CRP lags furthest behind at 6-8 hours since it depends on IL-6-driven liver protein synthesis.
Why does IL-6 fall so much faster than CRP after treatment starts?
IL-6 has a plasma half-life of roughly 1 hour, so its concentration tracks the real-time rate of cytokine release and drops quickly once the inflammatory drive resolves. CRP has a comparatively long and stable half-life of about 19 hours, so its level mainly reflects cumulative hepatic synthesis and declines slowly even after the underlying stimulus has stopped.
When does combination biomarker testing improve sepsis diagnostic accuracy?
Combination testing adds the most value in two scenarios: early presentation (under 6 hours from symptom onset), where IL-6 may already be elevated while CRP and PCT have not yet risen, and the CRP diagnostic gray zone (roughly 20-100 mg/L), where CRP alone cannot reliably separate bacterial from non-bacterial causes and adding PCT improves specificity.
Is CRP still useful if procalcitonin is more specific for bacterial infection?
Yes. CRP's long half-life makes it a more stable trend marker for tracking cumulative inflammatory burden over several days, and it is cheaper and more widely available on existing lab platforms than PCT. Most clinical protocols use CRP for general inflammation screening and add PCT or IL-6 when bacterial specificity or early detection is the priority.
Does Sekbio supply antibody pairs for CRP, PCT, and IL-6 multi-marker panels?
Yes. Sekbio manufactures validated monoclonal antibody pairs for CRP, PCT, and IL-6, each pre-validated in sandwich immunoassay format for CLIA, FIA, and ELISA development. Explore the individual datasheets or discuss a combined sepsis panel through our antibody development services.